As you may have gathered, I quite like the film Apollo 13. It features geeks (like me), space, peril, a true story, Tom Hanks… what’s not to like?
When everything goes wrong on the Apollo spacecraft, mission control get all the experts into the room. The engineers who have made the spacecraft, the people who fly the spacecraft (well not literally; they were stuck on the broken one, the backup crew came to the meeting), the people who understand retrograde burns and orbit trajectories. The Flight Director locks the doors and doesn’t let them leave until they have a plan.

Each person in the room has their own area of expertise and inevitably, lots of questions. Once they have come up with a plan, if new information comes in, they change the plan accordingly.
To steal President Biden’s phrase, Zoë is on her own, individual “cancer moonshot“. We are so far off the NICE guidelines now that we are charting a course into uncharted territory.
Yes, some patients have also had the same treatments Zoë has had — maybe even in exactly the same combinations — but I think that each cancer case is unique, genetically unique and as discussed previously, brain tumours are heterogenous and like to mutate. These factors (alongside the blood brain barrier) make them, in my mind, one of the hardest nuts to crack. The German geneticist (and who Zoë has a slight crush on) thinks that oncologists should stop treating cancer based on which part of the body it is in, and more based on what she calls “driver mutations” — and of course in Zoë’s case you need to factor in brain penetration (ooooerrr, missus!).
I want to add that this doesn’t make protocols or guidelines ineffective for some cancer types, but for brain tumours I genuinely think that precise, personalised medicine is the way forward on a “Pathway to a Cure”. To bring that quote out again: “insanity is doing the same thing over and over again and expecting different results“.
Anyway, the last eleven days have been all about processing the news; spreading the news (via the internet — mostly to stop lots of difficult conversations) and coming up with a plan that Zoë is happy with. We might be a bit slower than NASA… but I think we are more fun!
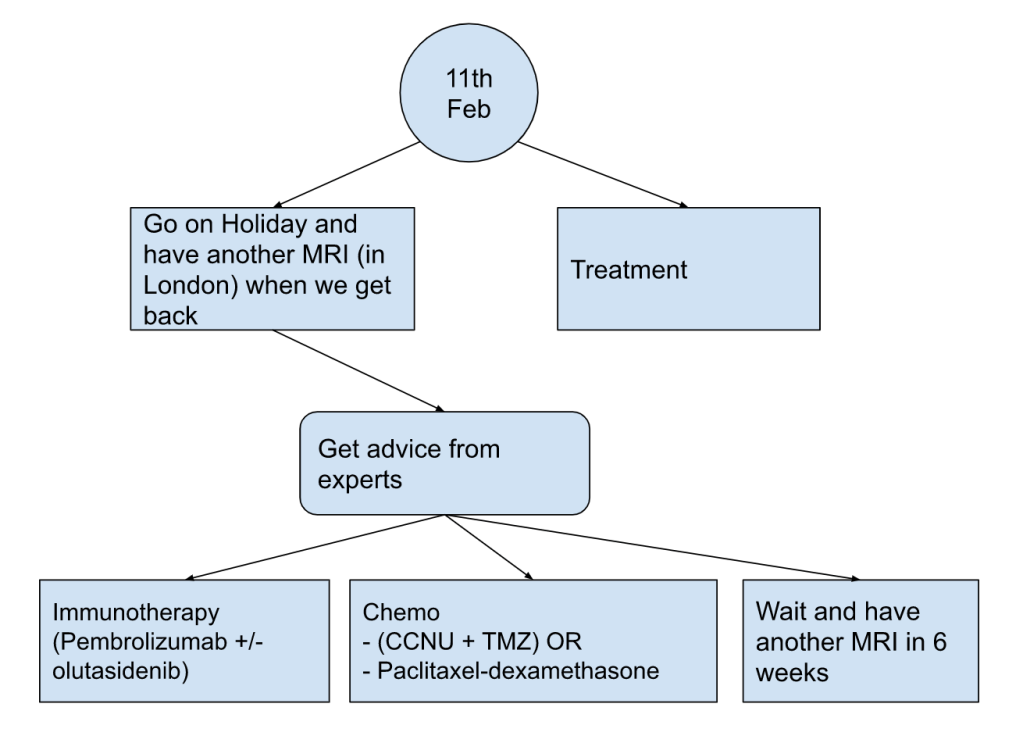
So what do we know so far: something doesn’t look right on the scan and we have got all the right experts in the room to come up with the plan, and, because I am involved we now have a flow chart.
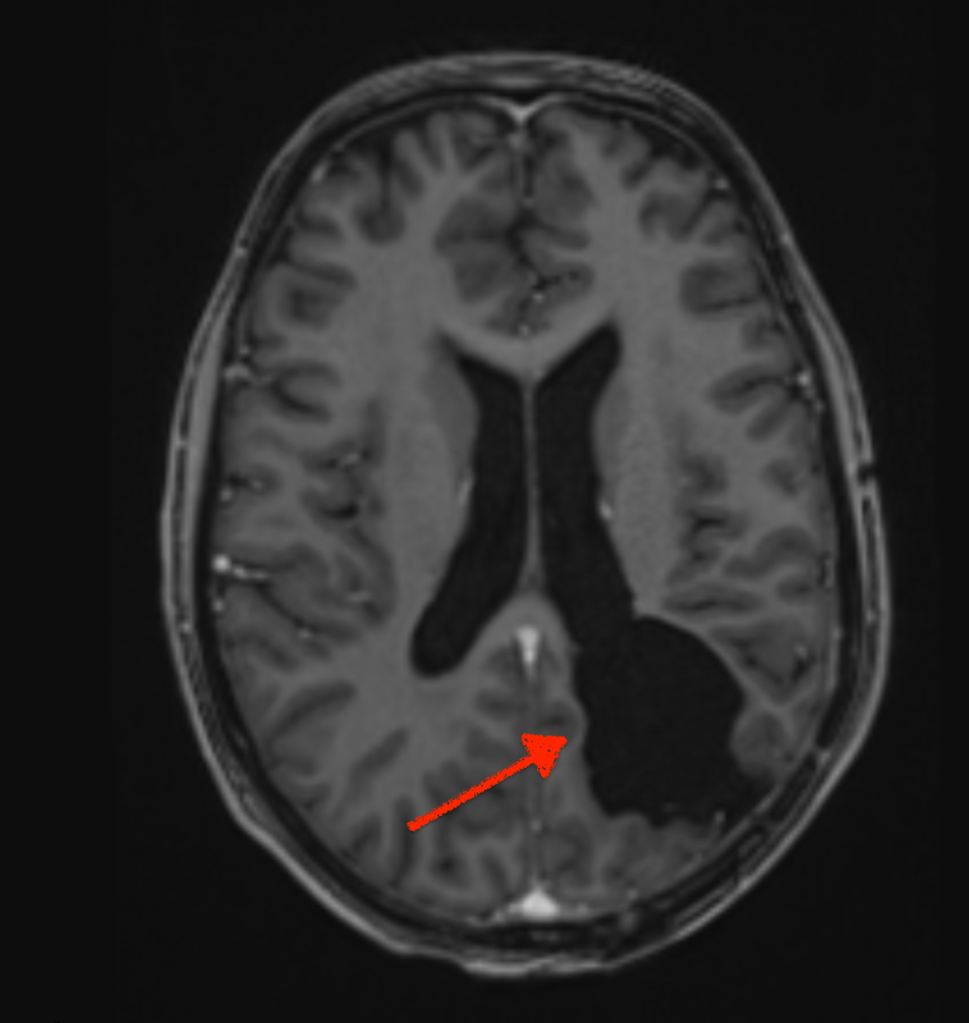
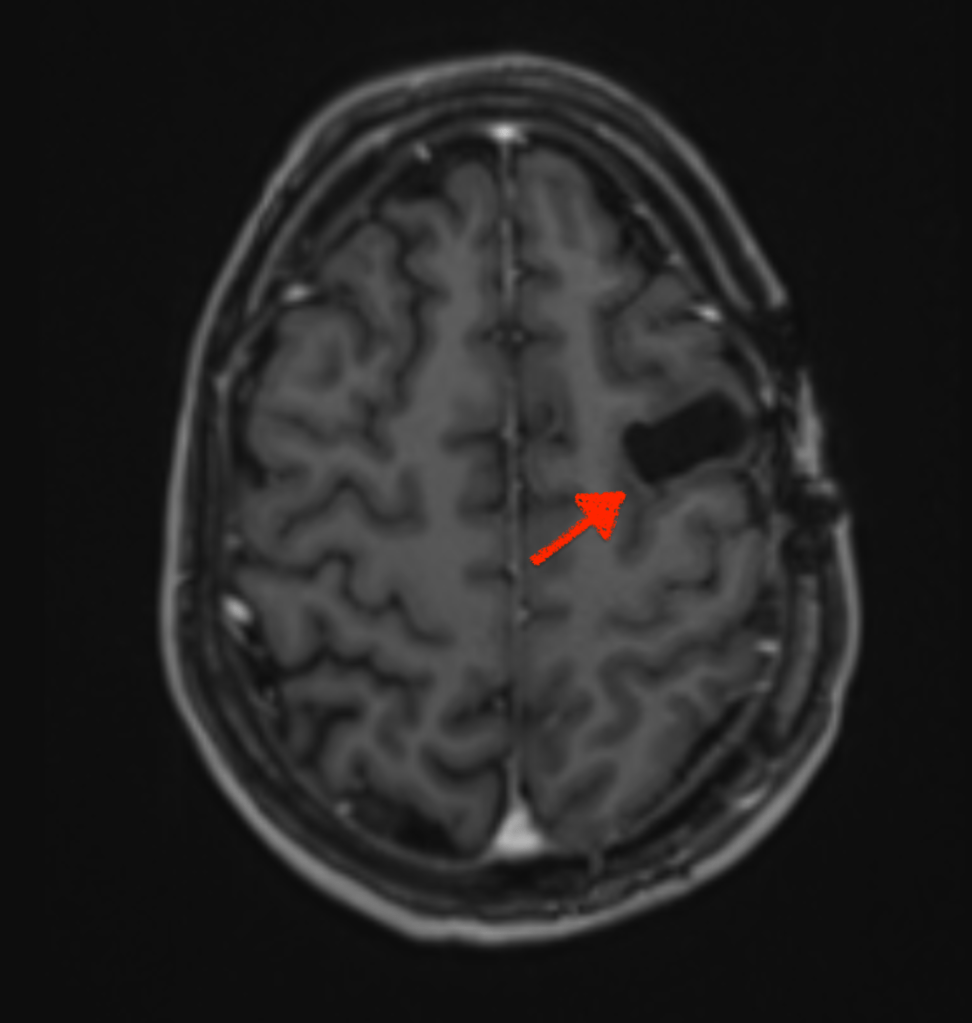
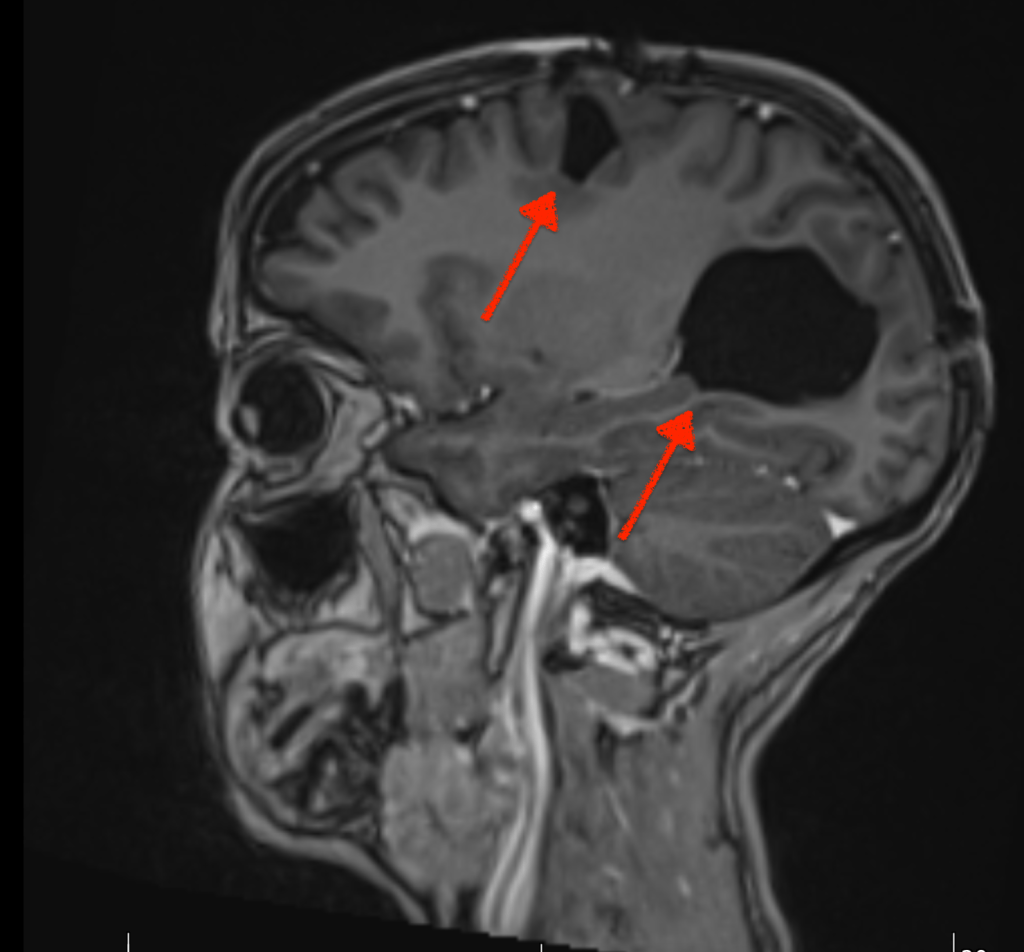
Zoë and only Zoë (as one of her oncologists reminded me) can decide. My role as advocate is to research treatments, make flow charts and advise her. She can, of course take advice from others; I guess doctors would be a good start. Sometimes, I have lost sight of her ability to make the right decision for herself; maybe focusing on the fact that she has had two chunks of her brain removed and acquired a brain injury in the process. Shocking as these images are, the surgeon may have removed the neurons that processes her right peripheral vision; but not her ability to make a decision. The brain is a fascinating organ.
Zoë has already made one decision: to go on holiday next week and not talk about cancer for the entire time we are there! This was the one thing that ALL the experts agreed on. I was once described as “solutions focused” (I think I put it in my LinkedIn bio), therefore my gut feeling was to do something right now— but sometimes in doctoring it seems waiting can be the right answer. I have to keep reminding myself that she is still currently having an active treatment: Optune, and she has spent the last > 12 months trying to train and boost her immune system to go out and fight the cancer!
She does need to make the next decision before we go away, to potentially allow the docs to file the “off-piste” paperwork in time. That decision is:
- Go “all in” with immunotherapy; double down, Vegas Style and pay for some really expensive drugs that could “supercharge” the vaccine and continue on her personal “moonshot”
- Go back to the tried and tested, reliable, dependable, understood but toxic chemo, that could potentially add some more “months”.
In order to make that decision, Zoë has to factor in her priorities, which she has stated to me are:
- Our children
- Quality not quantity of life
I’ve been told on multiple occasions by one of Zoë’s docs that I am “keen to pursue all possible strategies”. The inference is (maybe I am reading the room incorrectly), she is not. Well, he is right, I am, but I don’t think that pursuit is entirely without limits, or without Zoë’s priorities (see #1) — whenever I suggest a “wacky” treatment (ground essence of monkey poo) I have always assessed, in order of importance (to me, and hopefully Zoë):
- Toxicity to Zoë (not always clear)
- Risk vs Reward (not always clear)
- Toxicity to our bank balance (always clear)
Now there is plenty of “snake oil” out of there, and I think anyone pushing a treatment without solid statistical empirical evidence is frankly unethical. There is plenty of confirmation bias in cancer journeys. But if a patient wants to do something, surely that is up to them — it’s called “patient choice“.
My learned colleague Don reminded me of the case of a man with testicular cancer who wanted to achieve satori before he passed. He meditated (I would recommend Head Space – free if you have Vitality insurance like us) intensively, achieved both satori and remission. Is the moral of the story that enlightenment can overcome cancer? No. It’s that the guy was damned lucky and won the lottery.
Don’s comment about winning the lottery resonated me, when Zoë was first diagnosed I remember explaining to friends and family that she had “won one of the worst lotteries in the world”. We have been told (by a geneticist) that her cancer is not genetic, it is not down to lifestyle factors, it’s no one’s fault, it’s just sheer bad luck. Does this make it an easier cross to bear? Maybe, maybe not.
The NHS can’t offer treatments without assessing efficacy and cost effectiveness, they are a business at the end of the day, and they like all businesses don’t have a magic money tree.
For now our family need some space to allow Zoë to make the right decisions for her, and to do so, we are all (Zoë’s entire immediate family) getting on a plane to Fuerteventura!


Leave a comment